Tennis Elbow: Understanding the Pathology, Diagnosis, and Management of Lateral Epicondylitis
Introduction:
Tennis elbow, clinically known as lateral epicondylitis, is a common musculoskeletal condition characterized by pain and tenderness on the outer aspect of the elbow. Despite its name, tennis elbow is not exclusive to tennis players and can affect individuals engaged in various repetitive arm movements. In this article, we will delve into the pathophysiology, clinical presentation, diagnostic approaches, and current management strategies for tennis elbow.

Pathophysiology:
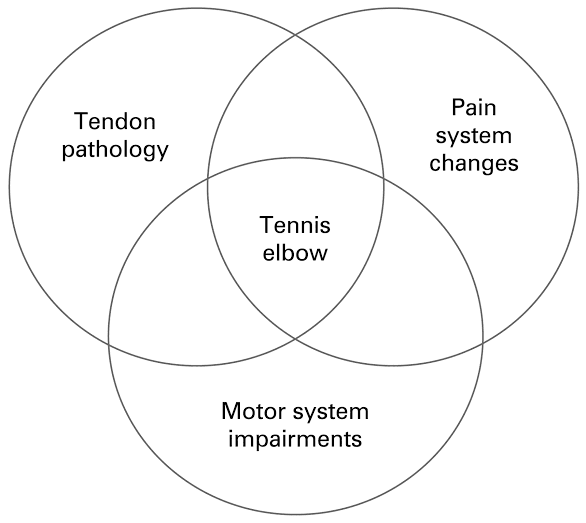
Tennis elbow primarily involves degeneration or microtears of the tendon fibers that attach to the lateral epicondyle of the humerus. These tendons belong to the extensor carpi radialis brevis (ECRB) muscle, which plays a crucial role in wrist extension. The repetitive and excessive use of the wrist extensors can lead to repetitive stress and strain on the tendon, resulting in a cascade of inflammatory and degenerative changes.
Clinical Presentation:
The hallmark symptom of tennis elbow is pain and tenderness located on the outer aspect of the elbow, specifically over the lateral epicondyle. The pain may radiate down the forearm, and individuals often experience difficulty with gripping, lifting, and performing activities that involve wrist extension. The pain is typically exacerbated by activities that stress the extensor tendons, such as gripping a racquet, turning a doorknob, or lifting objects.

Diagnostic Approaches:
The diagnosis of tennis elbow is primarily clinical and relies on a thorough history and physical examination. However, imaging studies are occasionally employed to rule out other causes of elbow pain or to assess the extent of tendon damage. Common diagnostic modalities include:
Physical Examination:
The healthcare professional will assess for tenderness over the lateral epicondyle, pain with resisted wrist extension, and pain with passive wrist flexion. These findings, along with a history of repetitive wrist movements, help establish the diagnosis.

Imaging:
X-rays are typically the initial imaging modality ordered to rule out bony abnormalities or arthritis. In some cases, magnetic resonance imaging (MRI) or ultrasound may be utilized to evaluate the integrity of the tendon, especially if surgical intervention is being considered or if the diagnosis is uncertain.
Management Strategies:
The management of tennis elbow involves a comprehensive and multimodal approach that includes both conservative and interventional strategies. The goal of treatment is to alleviate pain, promote healing, and restore function. The following management options are commonly employed:Conservative Management:
a. Rest and Modification of Activities:
Initially, reducing or avoiding activities that aggravate symptoms can help alleviate pain and allow the tendon to heal. Modifications in gripping techniques or using assistive devices may be recommended.
b. Physical Therapy:
Physical therapy plays a crucial role in the conservative management of tennis elbow. Therapeutic exercises, such as eccentric strengthening of the wrist extensors, stretching, and range of motion exercises, can help improve tendon healing and restore function.

c. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs):
Oral NSAIDs or topical NSAID creams/gels may be prescribed to reduce pain and inflammation. However, their long-term use should be monitored due to potential side effects.
d. Bracing or Splinting:
Wearing a counterforce brace or wrist splint can provide support to the extensor tendons and relieve stress on the affected area.

e. Extracorporeal Shockwave Therapy (ESWT):
ESWT involves the application of high-energy sound waves to the affected area, promoting healing and reducing pain. This modality has shown promising results in the management of tennis elbow.

Interventional Management:
a. Corticosteroid Injections:
Local corticosteroid injections are commonly used to provide short-term pain relief. However, their long-term efficacy and potential side effects should be considered, and repeated injections should be avoided.
b. Platelet-Rich Plasma (PRP) Injections:
PRP injections involve injecting a concentrated solution of platelets derived from the patient's own blood into the affected area. These platelets contain growth factors that promote tissue healing and regeneration.
c. Autologous Blood Injection:
This technique involves withdrawing the patient's blood and injecting it back into the affected area. The blood injection stimulates a healing response and can help alleviate symptoms.
d. Surgical Intervention:
Surgical options are considered when conservative measures fail to provide relief after a significant period of time. Common surgical procedures include debridement of the degenerative tendon, tendon repair, or release of the extensor origin.
Prevention and Rehabilitation:
Preventing tennis elbow involves employing proper techniques and equipment during activities that involve repetitive wrist movements. Strengthening the forearm muscles, using ergonomic equipment, and incorporating appropriate warm-up and stretching exercises can reduce the risk of developing tennis elbow. Following recovery, a gradual return to activities and continued rehabilitation exercises can help prevent recurrence.
Conclusions:
Tennis elbow, or lateral epicondylitis, is a prevalent condition characterized by pain and tenderness on the outer aspect of the elbow. Understanding the underlying pathology, clinical presentation, and appropriate diagnostic approaches is crucial for accurate diagnosis and effective management. A multimodal approach involving conservative measures, such as rest, physical therapy, and NSAIDs, is the mainstay of treatment. Interventional options, including injections and surgical interventions, are considered in refractory cases. By implementing preventive measures and appropriate rehabilitation, individuals can minimize the risk of tennis elbow and optimize their recovery. Early intervention and a comprehensive approach are key to achieving successful outcomes in the management of tennis elbow.



Comments
Post a Comment